I’ve been feeling crappy for a while.
Can I blame my awful, terrible allergies on my parents? Because I have always had awful, terrible allergies, and, yes, I have tried everything you’re going to suggest, from allergy shots to Allegra to local honey to non-dairy to acupressure to neti pots, to no avail. (Maybe it’s unfixable, and I just have to cope.) And cope I do, which is why I often have trouble distinguishing between the sort of crappy feeling that one dismisses as “allergies” and continues to slog through and the kind of crappy feeling that justifies, nay, necessitates lying in bed.
Add to that the fact that I generally assume I’m being a hysterical, hypochondriac faker, and you can see how it is that even as I held my newborn Graeme in my hands I had this sort of “no waaaay!” look on my face, like, “WOW! I wasn’t faking with all that shouting and grunting; I really was experiencing labor!”
I’m not even going to ask if I can blame this on my parents, because my mother already knows that I blame her ENTIRELY, and yet, do not love her any less for it. If anything, I love her more. If you can’t love the person who, at the age of 10, so convincingly faked an attack of appendicitis such that she persuaded a team of New York City surgeons to remove her perfectly good appendix, thus making it seem that nearly anything could be faked, and quite persuasively, too, really, who can you love?
So, anyway, a few days ago, it became clear that the unbearable pressure in my head and constant nausea was in fact a sinus infection, and that it had gone on long enough. I will allow as how I am one of those people who does, in fact, try things like swallowing whole cloves of garlic before running to the doctor, but when things get to the point of CANNOT LIFT HEAD OFF PILLOW WITHOUT WANTING TO PUKE, I’m like, hand me the ciprofloxacin, STAT.
{An aside, but please read it or the end of the post won’t make sense: as someone who does support the notion that women and families should have the choices to birth as ‘normally’ as possible, if that is their wish, I do NOT check all the boxes that homebirthy women often check off–anti-vaccine, anti-antibiotics–for the simple reason that I read a lot of history, often about disease. Sulfa, penicillin and vaccines are on our side in the Big Picture. It does not follow that every woman giving birth should have an enema, a shave, a disinfecting wash, and a constant drip of antibiotics into her veins, but it doesn’t mean that everything that modern medicine has wrought is bent on destroying your Birth Goddess moment. In fact, if you’re in a developed country, chances are you have the luxurious possibility of luxuriating in your ‘birth experience’ BECAUSE of the lovely, effective medications that would LOVE the chance to save your life should some Streptococcus or Mycoplasma have the audacity to invade your newly delivered nether bits, and because of the scientific progress that helped people understand why they oughtta wash their hands after dissecting cadavers before dealing wish those bits in a hospital context.}
I’m feeling much, much better now (thanks to above-mentioned ciprofloxacin) and ready to arise from my bed without barfing. Clearly, I need therapy that’s not pharmaceutical to figure out why I always just assume I’m faking it, but whatever.
As I was in the midst of this, one of my writing colleagues alerted me to this post (Peggy Orenstein on the sexualization of Candy Land on The Atlantic) in a way that suggested either excitement or distress. On reading it, at first I was like, “oh, how nice, some of my ideas and images made it onto The Atlantic!” And then I noticed that my name wasn’t there, nor any link to my blog (this has since been addressed.) And then, because I’m me, I wondered if I was FAKING, making it all up; if, in fact, this was an incredible coincidence and I had somehow been inspired by Peggy Orenstein without having ever read a word of hers or heard her speak and so on.
So I made a chart. I talked to this friend and this wise colleague and some other friends, and, of course, my resident scholar.
Am I just being crazy? I asked everyone.
I will leave the curious to explore Jana’s post and Ellen’s post as they choose, and I have but little else to say on the matter except that in the course of discussing this with others, I’ve discovered that (sometimes unintentional) borrowing and bold-faced plagiarism happens WAY more often than many of us suspect.

I’ve also discovered that it is a thankless job to point out such things (which is why I am profoundly thankful to Ellen and Jana) and, while one or more of us involved have been accused of trying to “self-promote,” the MORE LIKELY SCENARIO is that when people “blow the whistle,” so to speak, others will view them as–well, as ethical hypochondriacs–as people who are attempting to con surgeons into removing perfectly good organs; people who want to turn hay-fever into influenza; to take antibiotics for their allergies.
Look, I’m under no illusions that Jana and Ellen are Woodward and Bernstein, or that this little incident matters much at all in the HUGE scheme of things, except that it does, and here’s why: because if telling the whole truth matters in Big Things, it matters in little things. If it matters on the front pages of the New York Times it matters on little tiny blogs like this one. Women dying by the thousands and millions from puerperal fever wasn’t God’s punishment for immorality, as people suspected. It wasn’t from a Big Thing. It was from the tiny streptococcal spooks that people didn’t even know they should care about. And yes, the discovery of antibiotics helped, but just WASHING HANDS did, too.
And so I’m feeling less and less crappy, thanks not only to the cipro, but to those who risked being called ethical hypochondriacs, risked contaminating their hands enough to raise some questions as to whether the invisible spooks–the bacterium–of untruth had tainted my work, and to insist that those who write keep their hands clean of unintentional borrowing.
It’s not the kind of thing that earns a Nobel or any other kind of prize, but, then, neither was the hospital handwashing station, or the bar of soap.
Addendum: This is as good a place as any to say that both Ellen’s book, No Easy Choice, and Jana’s most recent book, Flunking Sainthood, deserve a place on your Amazon or indie bookstore wishlist, or, at the very least, on your library’s loan request system. I’ve written about both before on this blog (Ellen’s here; Jana’s here) but as usual I have more to say:
- Ellen’s book is absolutely a must read for people of faith dealing with infertility, the possibility of using techniques like in vitro fertilization (IVF) and genetic screening. It is a meticulous exploration of bioethics that’s written in a way that everyone can understand AND that shares her own story of living with a genetically caused disability and fearing passing on that disability to her children. As a meditation on human limitations and disabilities, it’s great. As a book on the questions facing those with infertility and other issues, it’s great. Essential, really. So, buy Ellen’s book.
- Jana’s book is laugh-out-loud funny in that vulnerable yet serious way of Anne Lamott, with the observational humor of a David Rakoff or a David Sedaris. But it is also a fantastic, entertaining look at many of the spiritual disciplines that people of faith (particularly Judeo-Christian faith) have followed for millenia, and all the more engaging because Jana actually did these disciplines, a different one each month, with mixed success. And if you should come across the fact that Jana is Mormon as you search for this book online, DO NOT TELL ME OR EVEN THINK that if you are evangelical, Anglo-Catholic, Catholic, or some kinda Reformed or Baptist Christian, that she has nothing to say to you. Her book is BIG TENT in the best sort of way, which is to say, it’s very much about seeing spiritual disciplines as a way to live like Jesus. It’s fabulous. So, buy Jana’s book.
Like this:
Like Loading...
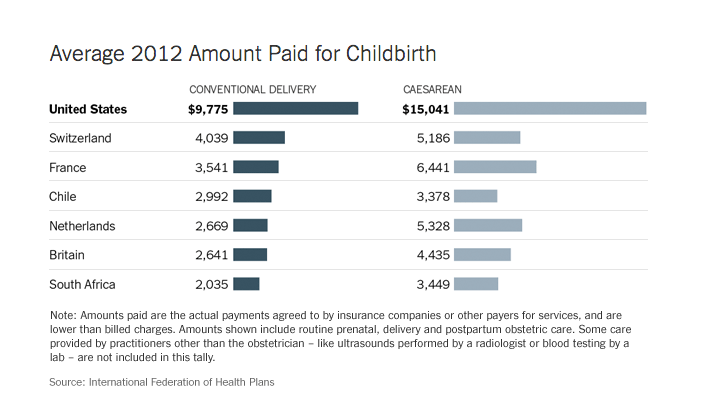
 I suppose one could justify the extraordinarily high cost of maternity care in the United States if the United States had corresponding extraordinarily high rates of maternal and infant health.
I suppose one could justify the extraordinarily high cost of maternity care in the United States if the United States had corresponding extraordinarily high rates of maternal and infant health.


